We use cookies to understand how you use our site and to improve the overall user experience. This includes personalizing content and advertising. Read our Privacy Policy
Accept Cookies
 info@cd-genomics.com
info@cd-genomics.comTumor Mutation Burden (TMB) is a key biomarker used to predict immunotherapy responses in different types of solid tumors, with higher TMB levels often indicating better outcomes due to increased neoantigen presence. It's clinical relevance extends to cancers like NSCLC, CRC, and melanoma, aiding in personalized treatments with both immunotherapy and targeted therapy options. Case studies across cancer types highlight TMB's value in stratifying patients and optimizing therapy choices, establishing it as a foundational tool in precision oncology.
TMB is a measure of the number of genetic mutations present within a tumor, typically expressed in mutations per megabase (mut/Mb) of DNA. Essentially, TMB reflects how much a tumor's DNA has been altered, with higher TMB levels indicating that the tumor has accumulated numerous mutations. The development of TMB as an biomarker, as discussed in the study by Chan et al. (2019)1, has been a critical advancement in oncology. Initially, TMB was recognized for its potential due to the high number of mutations present in some tumors, which was thought to increase immune recognition. Over time, researchers discovered that a higher TMB often correlates with improved responses to immune checkpoint inhibitors (ICIs).
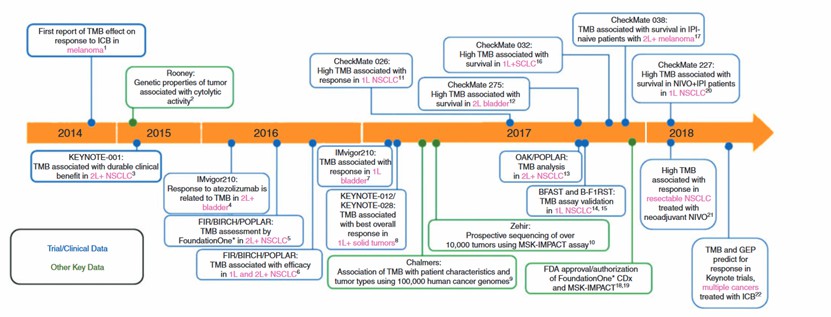 The evolution of TMB as an immunotherapy biomarker (Chan, T. A. et al,2019)
The evolution of TMB as an immunotherapy biomarker (Chan, T. A. et al,2019)
High TMB levels often indicate an increased presence of neoantigens which make tumors more recognizable to the immune system, then can lead to a more robust immune response. Consequently, tumors with high TMB levels allowing ICIs to attack cancer cells more effectively2.
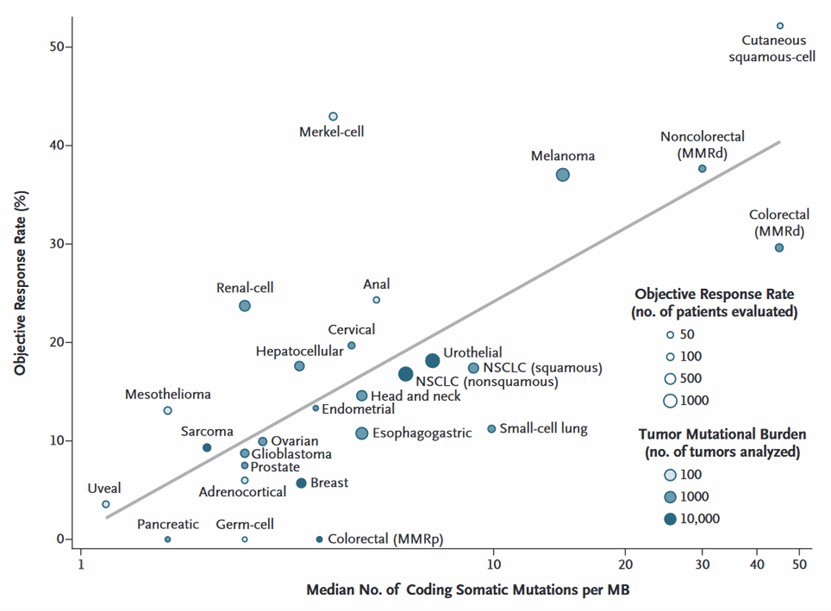 Correlation between TMB and Objective Response Rate
Correlation between TMB and Objective Response Rate
(Yarchoan, M.et al.,2017)
CD Genomics leverages cutting-edge sequencing platforms to provide comprehensive insights into tumor mutational burden, enabling detailed genetic profiling across solid tumors.
High TMB indicates a greater number of somatic mutations within the tumor genome, leading to the emergence of neoantigens which are crucial in rendering tumors more immunogenic, making them more likely to be targeted by T-cells. As a result, tumors with high TMB are often more responsive to immunotherapies, as the diverse neoantigen profile facilitates immune system recognition and attack.
Clinical studies have shown that high TMB is particularly associated with better immunotherapy outcomes in cancers. A study published in Genome Medicine highlighted that NSCLC patients with high TMB had a significantly higher objective response rate (ORR) to pembrolizumab compared to those with low TMB3. Similarly, in melanoma, patients with higher TMB show improved responses to anti-CTLA-4 therapies, as demonstrated in research published in New England Journal of Medicine4.
The clinical significance of TMB in predicting immunotherapy efficacy is further underscored by regulatory approvals. The U.S. Food and Drug Administration (FDA) approved pembrolizumab for TMB-high solid tumors across different cancer types, making TMB one of the first pan-cancer biomarkers in immunotherapy. This approval highlights TMB's role in patient stratification and its potential to optimize treatment plans. TMB's predictive power has also encouraged ongoing research into refining TMB measurement methods and defining TMB thresholds that align with optimal responses in various cancers, enabling more tailored immunotherapy strategies in oncology.
TMB is traditionally associated with predicting immunotherapy responses, but recent studies suggest it could also be valuable in identifying patients who may benefit from targeted therapies. Targeted therapies, which include drugs designed to interfere with specific molecules or pathways driving cancer progression, could be more effective in patients with certain TMB levels. This potential stems from the insight that high TMB often reflects the presence of numerous genetic alterations, some of which may affect critical oncogenic pathways or create new therapeutic targets within the tumor cells. This understanding has expanded TMB's role beyond immunotherapy into the realm of targeted treatments, especially in solid tumors like lung, bladder, and breast cancers.
High TMB in specific cancers has been associated with mutations in oncogenic drivers or DNA repair pathways, making such tumors more responsive to targeted inhibitors. For instance, tumors with mutations in genes involved in DNA damage repair (e.g., BRCA1/2, ATM, or mismatch repair genes) exhibit high TMB and are often sensitive to PARP inhibitors, which target the DNA repair process itself. Studies indicate that high TMB can be predictive of better responses to PARP inhibitors across multiple tumor types, as it may indicate a dependency on residual DNA repair mechanisms that these inhibitors disrupt3. Similarly, tumors with high TMB often harbor mutations that activate the PI3K/AKT/mTOR or MAPK signaling pathways, making them candidates for inhibitors targeting these pathways. This has been observed in cancers like melanoma and certain subtypes of breast cancer, where high TMB tumors responded well to MEK and BRAF inhibitors, as shown in a study published in New England Journal of Medicine5.
Furthermore, high TMB may help identify patients likely to benefit from combination therapies that include both targeted drugs and immunotherapies. In certain solid tumors, combining ICIs with pathway-specific inhibitors (such as EGFR or ALK inhibitors) has shown promise in clinical trials, particularly in high-TMB patients who exhibit resistance to monotherapy approaches. This combination strategy aims to capitalize on both the neoantigen-driven immunogenicity from high TMB and the direct oncogenic pathway inhibition, thus enhancing treatment efficacy and overcoming resistance to single-agent therapies.
The exploration of TMB as a predictive biomarker for targeted therapy is ongoing, with researchers evaluating the precise mutation types and pathways affected in high-TMB tumors. As the understanding of TMB in targeted therapy selection grows, it holds promise in advancing personalized oncology, allowing clinicians to select optimal therapy regimens for patients based on both mutation burden and specific genetic alterations.
TMB has increasingly been recognized as a crucial biomarker for tailoring personalized treatment approaches across various solid tumors, including lung, breast, and colorectal cancers. Each of these cancers has distinct mutation profiles and therapeutic needs, which TMB can help address by enabling more precise therapy selections. In lung cancer, particularly non-small cell lung cancer (NSCLC), high TMB is associated with better outcomes from ICIs.
In breast cancer, TMB has been identified as particularly relevant for triple-negative breast cancer (TNBC), a subtype known for its limited therapeutic options and aggressive nature. High TMB in TNBC correlates with a heightened response to immunotherapy, as shown in trials involving pembrolizumab combined with chemotherapy. The KEYNOTE-355 trial, published in The New England Journal of Medicine, revealed that TMB was a predictive marker for response to pembrolizumab in TNBC patients, supporting TMB's utility as a tool for identifying patients likely to benefit from immunotherapy in breast cancer6.
Colorectal cancer (CRC) is another area where TMB has shown promise, particularly in tumors with high microsatellite instability (MSI-H), a condition that often accompanies high TMB. MSI-H tumors, due to defective DNA mismatch repair, tend to have high mutation burdens, making them more responsive to immune checkpoint blockade therapies. Research published in Science found that high TMB was predictive of better responses to pembrolizumab in CRC patients with MSI-H tumors. For these patients, TMB provides an added layer of specificity in selecting candidates for immunotherapy, offering new avenues for those who might not respond to traditional chemotherapy7.
TMB has proven to be a valuable biomarker in clinical oncology, with case studies across various cancers illustrating its role in guiding treatment decisions and predicting patient outcomes. One of the most impactful uses of TMB has been in non-small cell lung cancer (NSCLC). In a study conducted on patients with NSCLC, demonstrated that patients with high TMB had higher overall response rates and longer progression-free survival than those with low TMB. These findings support TMB's value in patient selection for ICIs, as well as its role in improving survival rates for NSCLC patients who qualify for this treatment based on their TMB levels.
In melanoma, a cancer type often associated with a high mutation burden due to UV exposure, TMB has been crucial in guiding treatment strategies with anti-CTLA-4 and anti-PD-1 therapies. For example, a landmark study in New England Journal of Medicine found that melanoma patients with high TMB levels had a significantly improved response to the CTLA-4 inhibitor ipilimumab, underscoring the potential of TMB as a predictive marker for immunotherapy efficacy in melanoma patients4.
Colorectal cancer (CRC) is another solid tumor type where TMB has shown clinical relevance, particularly in tumors with high microsatellite instability (MSI-H). MSI-H status, which often coincides with high TMB, has been used to predict responses to pembrolizumab, a PD-1 inhibitor, in metastatic CRC. A pivotal study highlights TMB's applicability beyond NSCLC and melanoma, making it a pan-cancer biomarker for immunotherapy response in tumors with high mutational burdens7.
References:

